Financial penalties for avoidable hospitalisations.
June 23, 2021
The 2020-25 Commonwealth-state hospital funding agreement requires the Independent Hospital Pricing Authority to consider penalties for excessive rates of potentially preventable hospitalisations. The new penalty would sit alongside existing penalties on states with higher-than-expected rates of adverse events in hospitals.
Potentially preventable hospitalisations are defined as those that can either be avoided or their rate reduced with good primary health care.
One category of potentially preventable hospitalisations is admissions for vaccine-preventable diseases such as measles, and this category should probably now be updated and expanded to include COVID-related admissions. Potentially preventable hospitalisations also include admissions for heart disease and other chronic conditions where a higher rate of admission is an indicator of weaknesses in primary care.
The definition is still somewhat crude - could a hospital admission that is so serious it leads to a 10-day stay really have been prevented with good primary care? However, since first proposed in Australia more than a quarter of a century ago, the rate of potentially preventable hospitalisations has become established as a widely used indicator of health system performance.
In 2017-18 there were about 750,000 potentially preventable hospitalisations, including 85,000 that were vaccine-preventable (mostly pneumonia and flu), 330,000 potentially preventable acute admissions (including dental conditions and cellulitis), and 345,000 potentially preventable admissions for chronic diseases such as asthma and chronic obstructive pulmonary disease.
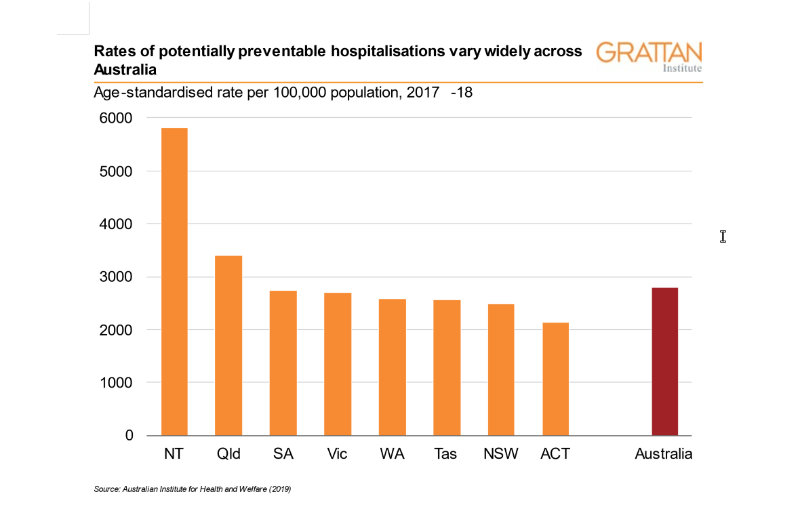
Potentially preventable hospitalisations occupied almost 3 million bed-days in 2017-18 and occurred at a rate of about 3,000 per 100,000 population. Some parts of Australia have much higher rates of potentially preventable hospitalisations than others (as shown on the graph below).
Who should be penalised for poor performance?
The task for the Independent Hospital Pricing Authority is a complex one. Potentially preventable hospitalisations are a measure of failures in primary care rather than hospital care, because by definition if the admission had been prevented the patient would not have gone to hospital.
The Commonwealth government is responsible for the system management and support, policy, and funding for GP and primary health care services, so any penalty for excess rates of potentially preventable hospitalisations should logically fall on the Commonwealth. But designing a penalty that falls on the Commonwealth without creating perverse incentives for the state will be tricky.
One approach could be for the Commonwealth to pay states for excess potentially preventable hospitalisations. This would require the Independent Hospital Pricing Authority calculating an expected rate of potentially preventable hospitalisation for each diagnosis on the potentially preventable hospitalisations list, adjusted for the factors that are known to lead to higher rates of admissions. The Commonwealth would then pay states the full costs of these higher-than-expected admissions in each diagnosis cluster.
But if this new higher payment for potentially preventable hospitalisations were passed on to hospitals, it would create a perverse incentive for hospitals to admit these patients inappropriately. Introduction of the new penalty should therefore be accompanied by an agreement with the states that they would not incorporate it into payments to hospitals. The states might also be invited to agree that any additional funding which flows to them should be used for state-wide programs to reduce potentially preventable hospitalisations or in areas with high rates of those admissions.
A new, reciprocal, and two-way penalty regime could also be used in other areas where failures in Commonwealth policy lead to higher costs in state hospital systems. New penalties on the Commonwealth might be for the costs of patients who have to remain in hospital after their acute care has been completed, because of long waits for aged care or appropriate accommodation under the National Disability Insurance Scheme.
Currently, the only penalties in Commonwealth-state agreements are for safety and quality of care breaches, and these fall on the states. Broadening penalties, so that some fall on the Commonwealth, would reflect more accurately the marble-cake nature of responsibility for healthcare in Australia.
